Personal Functioning and Engagement
The Personal Functioning and Engagement (PFE) implementation guide provides a structural framework that enables the FHIR-based exchange of information about an individual's ability to function in and engage with the world.
Introduction
Clinicians and caregivers describe and document the health and health-related state of individuals as a core activity of providing these indviduals appropriate care and support. Sharing the information collected - the details of the person's functioning in terms of body functions, activities, and participation - supports successful care coordination at transition of care and during on-going shared care. Care coordination - when a person transitions between healthcare settings, including ambulatory care, acute care, long-term post-acute care (LTPAC), and home- and community-based services (HCBS) - is often fragmented and can lead to poor health outcomes, increased burden, and increased costs. Interoperable health information exchange has the potential to improve patient and provider communication and supports access to longitudinal health information that enables improved efficiencies, higher quality of care, and better health outcomes. Data should be usable across the continuum of care, and beyond the traditional healthcare system - into the community.
Unfortunately, providers frequently do not receive complete and accurate information on patients transferred into their care in a timely manner, leading to adverse outcomes and additional expenses. This failure to exchange accurate, timely data often leads to inefficient workflows, duplicative data entries, and increased risk of patient harm attributable to missing or inaccurate information. Specifically within the post-acute care setting, poor quality discharge information is a major barrier to safe and effective transitions. With 45% of Medicare beneficiaries requiring post-acute care (PAC) services after hospitalization, the need for a seamless exchange of health information is great. The findings from a 2020 study highlight the significant gap in sharing information at transition. The survey assessed continuity between hospitals and skilled nursing facilities (SNF) and found that at transition of care complete mental status information was received by the SNF only 6% of the time. [JAMA Network Open. 2021;4(1):e2033980. doi: 10.1001/jamanetworkopen.2020.33980] .
Health Information Technology (Health IT) can significantly alleviate administrative burden by supporting health information exchange across care settings to ensure that the relevant information necessary to care for the incoming patient is delivered to the right person, at the right time - thereby improving patient outcomes, reducing provider burden, improving cost efficiencies, and improving workflows. Moreover, enhanced data exchange allows for advanced computability, standardization, usability, and real-time data analytics, enabling broader data use by health IT developers, researchers, providers, and payers.
Background
The Personal Functioning and Engagement Implementation Guide (IG) focuses on the representation and exchange of observations. The IG supports observations across many domains by drawing on the World Health Organization's (WHO) International Classification of Functioning, Disability and Health (commonly known as ICF), which defines health and health-related domains related to an individual's functioning from the perspective of the body, the individual, and society. Examples of domains that ICF defines that the IG can be applied to include but are not limited to:
- Mental functions captured as a part of evaluating an individual's cognitive status
- Mobility and Self-care captured as a part of evaluating an individual's functional status
- Communication, voice, and speech functions captured as a part of evaluating an individual's spoken language communication, swallowing, and hearing
More information on the concepts that may be included in this IG can be found in the ICF Browser
One impetus for this IG is the amendment to the Social Security Act in 2014 to include the Improving Medicare Post-Acute Care Transformation (IMPACT) Act. IMPACT requires the standardization and interoperability of patient assessment in specific categories for PAC settings, including long-term care hospitals (LTCHs), home health agencies (HHAs), SNFs, and inpatient rehabilitation facilities (IRFs). It focuses on the standardization of data elements in specified quality measure and patient assessment domains for cross setting comparison and clinical information exchange, respectively.
The Act requires:
- Reporting of standardized patient assessment data through commonly used PAC assessment instruments:
- Minimum Data Set (MDS)for SNFs
- Inpatient Rehabilitation Facility - Patient Assessment Information (IRF - PAI) for IRFs
- LTCH Continuity Assessment Record and Evaluation (CARE) Data Set (LCDS) for LTCHs
- Outcome and Assessment Information Set (OASIS) for HHAs
- Implementation of data elements specified in each domain using standardized data elements to be nested within the assessment instruments currently required for submission by LTCH, IRF, SNF, and HHA providers.
- Data to be standardized and interoperable to allow exchange of data between PAC providers, among others, using common standards and definitions to provide access to longitudinal information and facilitate coordinated care.
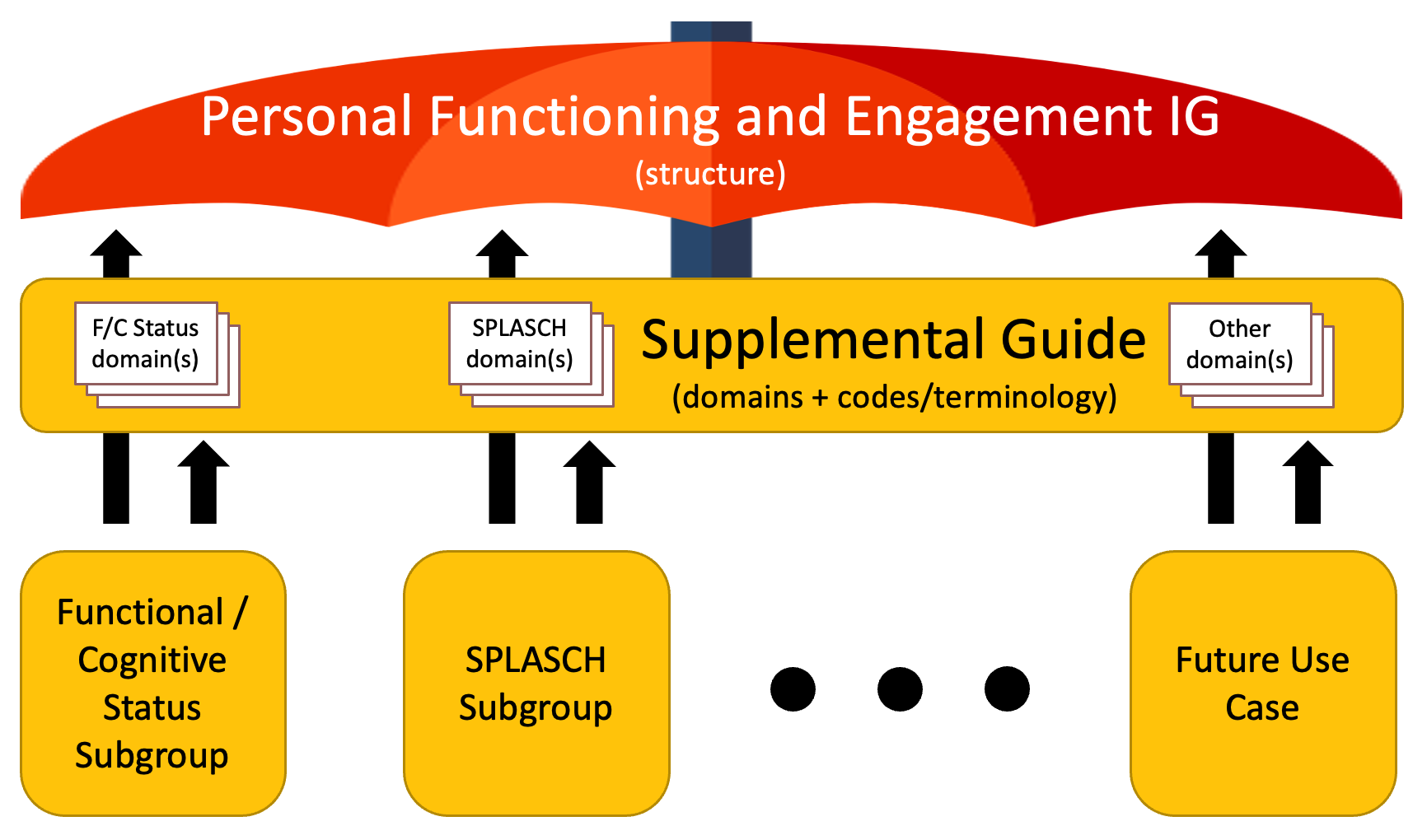
Personal Functioning and Engagement IG Structure